Zander AR et al. Gene Technology,Stem Cell and Leukemia ResearchNato Asi Series H: Cell Biology, Vol 94Springer-Verlag, Berlin Heidelberg New York London |
|
for St.-Petersburg BMT Center Team, 189646 St.-Petersburg Russia.
A significant proportion of patients, who did develop acute leukemia (AL) , chronic myelogenous leukemia (CML) , non Hodgkin-s (NHL) , Hodgkin-s disease (HD) , multiple myeloma (MM) , severe aplastic anemia (SAA) , myelodysplastic syndrom (MDS) and other malignancies may be cured with allogeneic (allo), autologous (auto) bone marrow and/or peripheral blood stem cell transplantation (PBSCT) .This article deals with first results of BMT and PBSCT performed at Petrov Research Institute of Oncology Table 1. GENERAL DATA ABOUT BMT TRANSPLANTATION
AT PETROV RESEARCH INSTITUTE OF ONCOLOGY 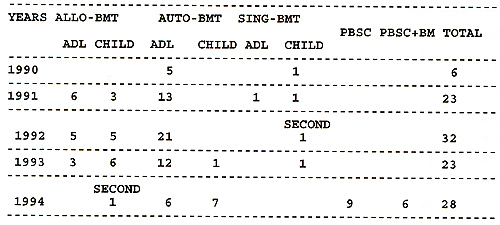
Table 2. PATIENT CHARACTERISTICS FOR ALLOGENEIC
BONE MARROW TRANSPLANTATION 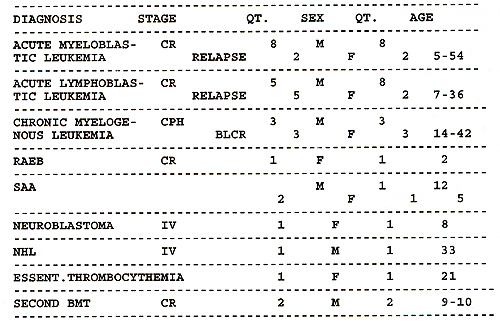
Table 3. PATIENT CHARACTERISTICS
FOR AUTOLOGOUS BONE MARROW TRANSPLANTATION  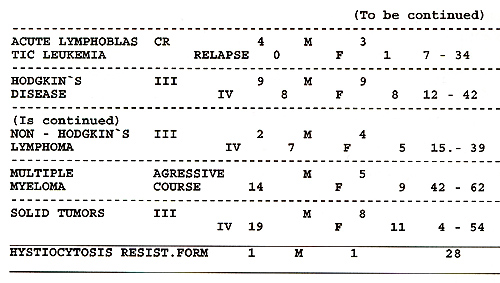
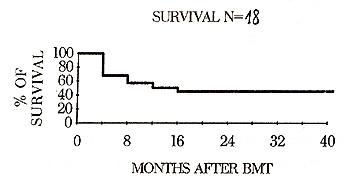
As seen from Table 1, an average of twenty-eight BMTs per year
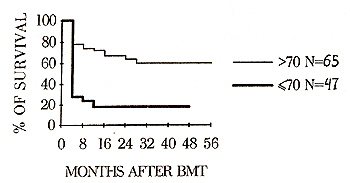
were performed at the St.- Petersburg BMT Center. Fig. 1 and 2 show
survival rates in the patients with AL and in patients with AML
treated with BMT. These results are in accordance with recent publications. 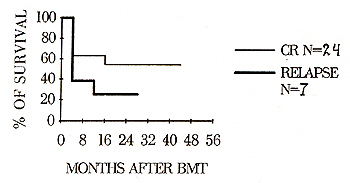 Fig.1 Survival rates in BMT patients
with AL
During the initial phase of transplantation program, we could not
strictly stick to the common eligibility criteria, and included
the patients with rather poor performance scores as well as with
other contraindications for BMT. Hence, initial results are to be
interpreted by considering an increased procedure-related mortality
(Fig.3) . The significant relapse rates are the main problem at
present time, due to changed inclusion criteria of patients.
Reasons of mortality after allo- and auto-BMT included clinical
relapses -30,3%, regimen-related toxicity -15,6%, acute GVHD -12,1%,
fatal septic infections -12,1%. The most important prognostic
factors for clinical outcomeof BMT were: patient age, Karnovsky
score, and stage of the disease at the time of transplantation
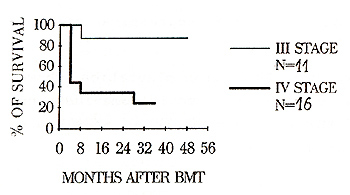
{Fig.3,4,5) . 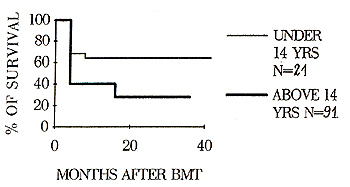
Fig.5 Survival of BMT patients with lymphomas (stage III vs. IV) Overall survival of patients with a pre-treatment
Karnovsky score of more than 70% were 62% {56 months follow-up)
, in children 65% {48 months follow up), in patients with AL {CR
state) 57 % {52 months follow-up) and and in patients with an early
stage of malignancy 85 % (50 months follow-up) , thus being much
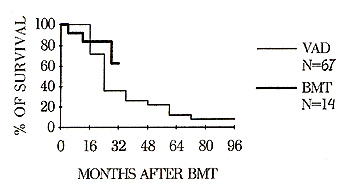
higher compared with other groups(p< 0.05) .Highdosage chemotherapy
followed by auto-BMT increased the overall survival rate in patients
with aggressive multiple myeloma (MM), compared to conventional
therapy, (62% during 32 months and 15% during 96 months, respectively,
p < 0,05) , as shown in Fig. 6.
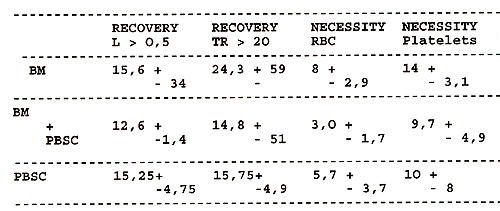
Table 4. BLOOD RECOVERY (days) AND REQUIREMENT
FOR BLOOD PRODUCT TRANSFUSION When summarizing the aforementioned data, a conclusion may be drawn, that the latest experience of St.-Petersburg BMT Center yielded sufficient clinical results which are in good agreement with results of multicentric studies. One of the most promising approaches will be the wider use of intensive chemo/radiation therapy employing hematopoietic stem cells transplantation. Treatment should be started at the earliest stage of malignancy, especially in patients with poor prognosis. 
We would like to express our deep gratitude to Prof. Axel Zander and to all his colleagues at BMT Center, University Hospital Eppendorf (Hamburg), for valuable aid, clinical consulting and stimulating discussions. |